When and how to treat for lungworm
Wednesday, 3 May 2023


Weather will determine when clinical lungworm disease will be seen in herds. L3 can overwinter in the faecal pat and emerge when conditions are optimal >15-20°C can emerge as low as and damp/wet.
When do we see lungworm disease (hoose) in Ireland?
Weather will determine when clinical lungworm disease will be seen in herds. L3 can overwinter in the faecal pat and emerge when conditions are optimal >15-20°C can emerge as low as and damp/wet. L3 can often emerge en masse following rainfall and result in a larval explosion on the pasture. In Ireland, we typically see infective larval emergence in the summer months June and July, although there is considerable variation year to year. Wet summers are a high-risk factor for lungworm disease as the conditions will promote larval dissemination and high infective burdens.The journey from ingestion of L3 on pasture to migration through the blood and lymph and moulting for the L4 to reach the alveoli in the lungs takes approximately one week. Clinical signs will appear pre-patency from 8-25 days after grazing on infective pasture due to immature larvae in the lower airways.
In the milking herd, a milk drop will often precede clinical signs or occur when signs first develop in cows. Watching the milk tank closely is essential to detecting early choose. Variation in signs between individuals in a herd is common, ranging from no signs, some coughing, or dyspnoea. A cough with exercise when they are moving into the parlour is typically the first sign observed in individual animals. Approximately 1-2% of animals can develop a hypersensitivity to the nematode and this can lead to acute respiratory distress.
Cows have strong immunity to gutworms, why not lungworms?
Unlike gutworms, lungworm immunity has two parts: L4 larvae in the lower airways and adult worms in the bronchi. The immunity to incoming L4 larvae is only around 2 months. The immunity to adult Dictyocaulus is approximately two years.When adult cows go into housing and stop ingesting larvae, they lack exposure to developing larvae due to housing and cold temperatures will result in immunity waning. Because L4 in the lower airways cause prepatent disease and milk yield drops, treatment of adult cows is often necessary in Ireland.
Reinfection syndrome is caused by animals being put onto heavily contaminated pasture. If L4 immunity has waned over the dry and winter period, large numbers of migrating worms can reach the bronchi and elicit a strong immune response and hypersensitivity reaction characterised by eosinophilia and severe clinical signs such as acute dyspnoea.
This important variability is thought to originate from differences in the way each study was designed, from differences in GIN burdens, treatment protocols, drugs used, geographic locations and also from age group. This finding suggests that before advising a wormer to a particular herd, it is prudent to evaluate the risk of infection by cattle worm with the attending veterinarian.
How should we diagnose lungworms?
Lungworm is presumptively diagnosed based on the presence of a dry cough in animals on pasture in the summer months, usually accompanied or preceded by a milk yield drop. Due to the low infective burden and severity of clinical disease, it is considered urgent to treat. Other differentials include bacterial and viral infections such as IBR, PI3, RSV, Mycoplasma, and Pasteurella. The presence of pyrexia and oculonasal discharge would raise clinical suspicion of a viral and/or bacterial disease.As prepatent disease will cause clinical signs, faecal testing (Baermann faecal flotation) has very low sensitivity when managing early signs in calves and cows.
Milk bulk tank ELISA antibody testing requires 30% herd prevalence to achieve a positive titre, which indicates herd exposure. The test detects antigen to adults, so it does not detect prepatent disease. Additionally, antibody levels do not increase significantly until four to five weeks after exposure, leaving a very large gap in detection and making antibody testing not a useful diagnostic tool.
Bronchoalveolar lavage (BAL) is the best diagnostic method to detect prepatent disease. Larvae can be grossly and microscopically visualised, although sensitivity is still low. Larvae would be expected to be seen in 1:6 cows if there is a lungworm disease within the herd. For this reason, BAL should be performed on six clinical cows no matter the size of the herd. The presence of >4.7% eosinophils in the BAL fluid analysis is the most accurate diagnostic criteria for lungworm infection at >85% sensitivity and specificity (see Fig). It is important to note that eosinophils can remain elevated following initial exposure to lungworm larvae for up to 3 months following infection, so their presence on fluid samples taken after treatment or initial exposure does not conclude reinfection.
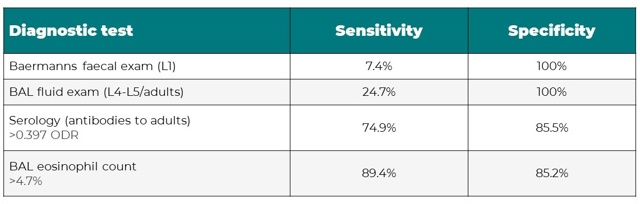 Source: Lurier T, Delignette-Muller ML, Rannou B, Strube C, Arcangioli MA, Bourgoin G. Diagnosis of bovine dictyocaulosis by bronchoalveolar lavage technique: A comparative study using a Bayesian approach. Prev Vet Med. 2018 Jun 1;154:124-131.
Source: Lurier T, Delignette-Muller ML, Rannou B, Strube C, Arcangioli MA, Bourgoin G. Diagnosis of bovine dictyocaulosis by bronchoalveolar lavage technique: A comparative study using a Bayesian approach. Prev Vet Med. 2018 Jun 1;154:124-131.
For a video on how to complete a BAL featuring Eoin Ryan, BVetMed, DipECBHM, UCD School of Veterinary Medicine:
When should we treat and what cows should we treat?
The presence of a seasonal dry, non-productive cough, particularly noticeable when cows are moved is enough to reach a presumptive diagnosis of lungworm. Due to the severe welfare consequences of the disease, treatment is indicated at the onset of signs and it should not be delayed to pursue diagnostics. Additionally, available testing with Baermann feacal and milk ELISA antibodies only detect patent disease, which leaves a gap in diagnosis as coughing begins with prepatent disease.Sustainable anthelmintic management involves leaving an untreated portion of refugia to slow resistance development and targeting animals for treatment. For lungworm disease, animal welfare supersedes this sustainability practice, and it is recommended to blanket treat the herd when the first signs of lungworm disease are observed in individual cows. They are all presumed exposed to the same burden with disease consequences, so aggressive management to prevent severe disease consequences is warranted.
Animals should always be assessed for the presence of other disease such as viral and bacterial disease that may result in mucoid oculonasal discharge, pyrexia, or worsening or persistent clinical signs despite anthelmintic treatment.
Currently, there is not any anthelmintic resistance documented with Dictyocaulus. All anthelmintics are effective against L4 and adult lungworm; however, only macrocytic lactones have the residual activity to prevent reinfection for a period. Eprinomectin is the only anthelmintic with zero milk withdrawal, making it a unique and economic treatment option for the milking herd.
Eprecis®: The only injectable eprinomectin for lungworm treatment
Two formulations are available of eprinomectin to manage lungworm in the milking herd: pour-on and injectable. Eprecis® is the only injectable form of eprinomectin on the market, making it a precise, reliable, and sustainable option for lungworm treatment.
Injectable Eprecis® will not be impacting by extrinsic factors such as licking, weather, or coat debris. Licking can heavily impact bioavailability of pour-on formulations, resulting in a risk of sub-dosing. Sub-dosing is a primary driver of anthelmintic resistance, so treating with Eprecis® not only ensures an accurate and reliable dose is received by the animal, but also promotion of responsible anthelmintic use.
Click here to buy Eprecis.
*References available upon request.